If emergency healthcare handles ePHI, I treat encryption as the default. HIPAA may label encryption “addressable,” but in practice, emergency departments, EMS teams, trauma programs, telehealth platforms, and vendors should encrypt data at rest and in transit if they want to cut breach risk and avoid painful reporting after a lost device.
Here’s the short version:
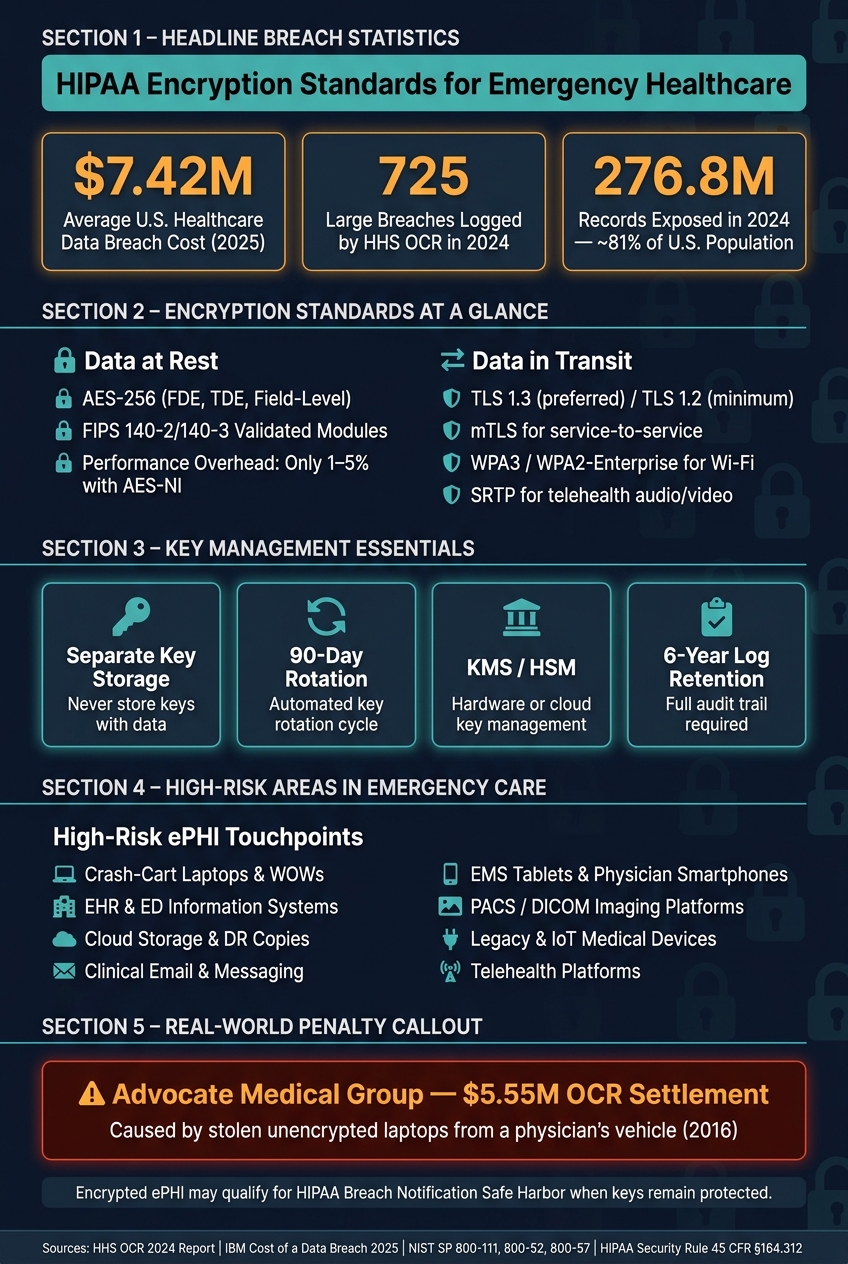
- I use AES-256 for stored ePHI on laptops, tablets, servers, databases, backups, and cloud copies.
- I use TLS 1.3 where possible, or hardened TLS 1.2, for ePHI moving across APIs, portals, email systems, telehealth tools, and internal services.
- I keep encryption keys separate from the data and manage them through KMS or HSM tools.
- I expect FIPS 140-2/140-3 validated modules and NIST-based key handling.
- I treat mobile devices, shared workstations, PACS, EHRs, backups, Wi-Fi, and third-party vendor links as high-risk areas.
- I document break-glass access, test restores, rotate keys, and keep audit logs for 6 years.
- I do not assume an emergency waives security duties. It does not.
A few numbers make the point fast:
- A U.S. healthcare data breach cost an average of $7.42 million in 2025
- HHS OCR logged 725 large breaches in 2024
- Those breaches exposed about 276.8 million records
- Advocate Medical Group paid $5.55 million after stolen unencrypted laptops led to OCR action
HIPAA Encryption Standards for Emergency Healthcare: Key Stats & Benchmarks
HIPAA Security Rule
sbb-itb-535baee
Quick comparison
| Area | What I look for | Common use |
|---|---|---|
| Data at rest | AES-256, FDE, TDE, field-level encryption | Laptops, EMS tablets, EHR databases, PACS, backups |
| Data in transit | TLS 1.3 or TLS 1.2, mTLS, SRTP, WPA3 | APIs, portals, telehealth, messaging, Wi-Fi |
| Keys | Separate storage, rotation, KMS/HSM, envelope encryption | Cloud, backups, database systems |
| Legacy devices | Isolation, VPN, IPsec, encrypted network segments | Older medical and IoT devices |
| Governance | Risk analysis, BAAs, log retention, restore testing | Internal systems and third-party vendor risk management |
So if I had to sum up the whole article in one line, it would be this: encrypt everything that stores or moves emergency ePHI, prove it works, and make sure vendors meet the same bar.
HIPAA Encryption Requirements and Regulatory Foundations
HIPAA Security Rule Provisions for Data at Rest and in Transit
Two HIPAA Security Rule provisions deal with encryption. 45 CFR §164.312(a)(2)(iv) applies to data at rest, which means encrypted storage on systems, devices, and media. 45 CFR §164.312(e)(2)(ii) applies to data in transit, which means protecting ePHI while it moves from one place to another.
HIPAA requires covered entities and business associates to assess encryption for ePHI at rest and in transit under 45 CFR §164.312. In day-to-day terms, that makes encryption the default safeguard for most emergency healthcare systems.
Those rules start with HIPAA, but the day-to-day setup comes from NIST and FIPS standards.
NIST and FIPS Guidance That Shapes HIPAA-Aligned Encryption
HIPAA sets the duty. NIST and FIPS show what that looks like in practice.
For emergency healthcare organizations, a defensible baseline includes:
- NIST SP 800-111 - Strong, FIPS-validated encryption for stored data
- NIST SP 800-52 - TLS 1.3 preferred, with TLS 1.2 as the minimum for data in transit
- NIST SP 800-57 / FIPS 140-2/3 - A documented key management and rotation policy that uses validated cryptographic modules; keys must never be stored alongside the data they protect [8][9]
The HITECH Act amendment (HR 7898) gives organizations one more reason to stay close to NIST standards. If an organization can show 12 months of compliance with a recognized NIST framework before a violation, it may qualify for reduced OCR penalties or a shorter audit [7][9].
Emergency Declarations, Minimum Necessary, and Secure Sharing
Emergency conditions can change how people work, but they do not remove the encryption duty. During declared emergencies, some Privacy Rule requirements may be relaxed, but the Security Rule still applies [3][10]. Disclosures must still follow the minimum necessary standard [3]. And contingency plans under 45 CFR §164.308(a)(7) need to keep encryption in place during disruptions [7][3].
The next section looks at how these rules apply to specific emergency healthcare systems and storage environments.
Encryption Standards for Emergency Healthcare Data at Rest
Core Encryption Standards for Endpoints, Servers, Databases, and Backups
Use AES-256 with FIPS 140-2/140-3 validated modules for ePHI at rest [1][5]. The good news is that modern processors help keep the hit small. With AES-NI, performance overhead is usually just 1% to 5% [11].
The right encryption layer depends on the system in front of you. Full-disk encryption (FDE) is the standard choice for endpoints like laptops, tablets, and mobile devices. On servers, Transparent Data Encryption (TDE) protects database volumes. For the most sensitive fields, such as Social Security Numbers, Medical Record Numbers (MRNs), and clinical notes, field-level encryption adds another shield on top of TDE. That matters because it can still protect those values if an attacker gets valid database credentials.
Backups need the same care. Encrypt them before they go to cloud storage, and keep backup keys under your organization's control.
Key handling matters just as much as the algorithm. Store keys separately from the data they protect. Use a KMS or HSM for storage and rotation. Envelope encryption makes this far easier to manage: a Data Encryption Key (DEK) encrypts the data, and a Key Encryption Key (KEK) encrypts the DEK. That setup supports automated rotation every 90 days without forcing teams to re-encrypt huge datasets [5].
You also need a paper trail. Log every encryption and decryption event with the user ID, timestamp, and key ID, and retain those logs for six years [5].
The risk to patient care isn't abstract. In 2016, Advocate Medical Group paid a $5.55 million OCR settlement after unencrypted laptops were stolen from a physician's vehicle [3].
Emergency Systems That Require Encryption by Design
In emergency care, encryption can't be bolted on later. ePHI moves through a messy, fast-moving mix of devices and systems, so protection has to be built in from day one.
Crash-cart laptops and workstations on wheels (WOWs) are easy to move and easy to lose. They should use FDE with pre-boot authentication managed through MDM. The same goes for EMS tablets and physician smartphones used for clinical communication or EHR access.
On the server side, EHR and ED information systems should run TDE on database volumes, with field-level encryption layered onto the highest-sensitivity data. Imaging platforms like PACS and DICOM systems hold massive amounts of diagnostic data, so every disk volume, snapshot, and archive copy should be encrypted.
For cloud-hosted environments, encryption has to cover object storage, database snapshots, and disaster recovery copies. And here's the part many teams miss: the organization should keep control of the keys instead of leaning on default cloud-provider key management.
A simple way to cut risk is to reduce local ePHI caching wherever possible. If local caching can't be avoided, that cache should be encrypted. And for legacy devices that can't run modern encryption? Don't leave them exposed on the open network. Isolate them behind encrypted tunnels such as VPN or IPsec.
Storage Encryption Methods Compared for Emergency Workflows
Each method protects against a different kind of failure or attack. The table below ties those methods to emergency-care use cases, which makes weak spots easier to spot.
| Encryption Method | Typical Emergency Use | Security Strength | Performance Impact | Implementation Complexity | Best-Fit Scenario |
|---|---|---|---|---|---|
| Full-Disk (FDE) | Crash-cart laptops, WOWs, EMS tablets | High - protects against physical theft | Negligible | Low - OS-native tools like BitLocker | All portable endpoints and mobile devices |
| Database (TDE) | EHR systems, ED information systems, imaging platforms | Medium - protects against disk theft | Minimal | Medium - requires vendor support | Protecting entire data volumes on servers |
| Application/Field-Level | SSNs, MRNs, clinical notes within shared databases | Very high - protects against SQL injection and credential compromise | Moderate | High - requires code or configuration changes | High-sensitivity fields in cloud or shared databases |
| Backup/Archive | Offsite snapshots, cloud archives, disaster recovery copies | High - protects historical data from exfiltration | Low | Medium - requires key separation | Long-term clinical record retention and DR copies |
The safest setup uses layers, not a single control:
- FDE for endpoints
- TDE for servers
- Field-level encryption for sensitive data
- Separate encryption for backups
These controls focus on data at rest. Transit encryption handles protection while data moves between systems.
Encryption Standards for Emergency Healthcare Data in Transit
Transport Security for Clinical Networks, APIs, and Interoperability
Once stored data is protected, the next job is securing ePHI while it moves between systems, staff, and devices.
In emergency care, that movement never stops. ePHI travels between triage tools, EHRs, imaging systems, messaging platforms, and remote responders. That means an attacker doesn't need much - just network access or one compromised hop. Under HIPAA, ePHI in transit should be encrypted, or covered by an equivalent safeguard.
Use TLS 1.2 or later, and lean toward TLS 1.3 for patient portals, FHIR APIs, telehealth, and internal service traffic [1][5]. TLS 1.3 is also faster than TLS 1.2 because it needs fewer round-trips during the handshake. SSL v2/v3 and TLS 1.0/1.1 are outdated and open to attack, so turn them off at the load balancer or gateway level [1][5].
Cipher suite choice matters just as much. Good options include AES-256-GCM or ChaCha20-Poly1305, paired with ECDHE (P-256 or X25519) for key exchange [1][5]. ECDHE gives you forward secrecy. Put simply, if a private key gets exposed later, it still can't be used to decrypt old recorded sessions.
For FHIR APIs and other interoperability interfaces, require HTTPS with TLS 1.3 on every endpoint. For internal service-to-service calls, mutual TLS (mTLS) adds another check by making both sides present certificates. Use automated certificate rotation and short-lived certificates. Also enforce HTTP Strict Transport Security (HSTS) so clients don't quietly drop back to unencrypted connections [1][12].
Securing Email, Messaging, Telehealth, Wireless, and Connected Devices
Emergency care also depends on email, messaging, telehealth, and wireless access. Each channel needs its own transport control.
Use S/MIME or an approved secure email gateway to encrypt outbound ePHI. For clinical messaging, end-to-end encryption helps protect message content even from the platform provider, and the platform must still support retention and audit needs. For telehealth, use SRTP for voice and video streams, along with TLS 1.2+ for signaling [6][2].
For clinical Wi-Fi, run WPA3 or WPA2-Enterprise (802.1X/EAP-TLS) [1][14]. Skip pre-shared keys in clinical settings. If connected medical devices can't support modern encryption on their own, place them behind secure gateways or on encrypted segments. That way, the device can stay in use without opening up the network [1][12].
Transport Options in Emergency Communications Compared
The table below matches the right transport control to the right emergency workflow.
| Transport Option | Protocol/Standard | Latency Profile | Emergency Use Case | Common Misconfiguration Risk |
|---|---|---|---|---|
| VPN (IPsec/SSL) | AES-256, IKEv2 | Moderate | Remote access, site-to-site HIE transfers | Misconfigured split tunneling |
| TLS-Secured HTTPS | TLS 1.3, AES-GCM, ECDHE | Low | FHIR APIs, patient portals | Deprecated cipher suites or expired certificates |
| mTLS | TLS 1.2/1.3 + mutual certificates | Low | Internal service-to-service calls | Certificate expiration |
| Secure Messaging | End-to-End Encryption | Low | Clinical team coordination, EMS mobile texting | Lack of archival for records |
| Secure Email | S/MIME or secure gateway | Moderate | External consultations, lab results | User error sending ePHI unencrypted |
| Telehealth | SRTP + TLS 1.2+ | Low (real-time) | Emergency tele-triage, remote teleconsults | Unencrypted signaling or metadata |
| Wireless (Wi-Fi) | WPA3 / WPA2-Enterprise | Low | Mobile tablets and wireless monitoring devices | Weak pre-shared keys |
Encrypted ePHI can qualify for HIPAA safe harbor when keys remain protected [5][2].
Implementing, Governing, and Continuously Assuring Encryption
Once the standards are in place, the next job is making sure encryption still works when things go sideways: downtime, recovery, emergency access, and data shared with outside partners.
Designing Encryption for Availability, Break-Glass Access, and Incident Response
In emergency care, encryption has to protect data without getting in the way of clinical work. After the standards are set, the focus shifts to keeping encryption available during downtime, failover, and emergency access.
Start with a HIPAA-aligned risk analysis for every ePHI flow. Break-glass access is part of emergency care, so the process needs to be spelled out in plain terms. Require two approved custodians, and log every key access and decryption event with user ID, timestamp, and key ID [1][5]. After every patch, failover, and restore, verify that encryption still works and that backups can still be decrypted.
Third-Party Encryption Requirements, Assessments, and Policy Enforcement
Emergency care runs on vendor connections, which means encryption controls can't stop at your own systems. They need to extend to business associates and connected devices too. And those controls can't be taken on faith. Vendors need to show proof.
Put those requirements into BAAs and security addenda. Review SOC reports, test TLS settings, and confirm customer-managed keys for cloud-hosted ePHI. If a vendor can't prove compliance, block them [1][13].
Some medical devices still can't support modern encryption on their own. In those cases, the governance move is simple: isolate and segment them on encrypted VLANs with IPsec tunnels [11].
Using Censinet for Encryption Risk Management in Emergency Care
These controls only help if the organization can keep checking them across vendors and assets over time. Censinet RiskOps™ helps teams assess and track encryption controls across vendors, applications, devices, and supply chains.
The table below maps common emergency workflows to the encryption controls they need, where the risk tends to show up, and what governance teams should do about it.
| Workflow / Asset | Required Encryption Control | Key Risk Point | Governance Action |
|---|---|---|---|
| EHR / Databases | AES-256 (TDE) + field-level encryption | Over-privileged service accounts | Quarterly access and key rotation audit |
| Mobile / EMS Devices | Full-disk encryption (FDE) via MDM | Device loss or theft | Enforce remote wipe and biometrics |
| Medical / IoT Devices | Network-level VPN/IPsec tunnels | Legacy firmware with no native crypto | Segment on isolated encrypted VLANs |
| Cloud Services | Customer-managed keys | Provider access to master keys | Define key ownership in BAA |
| Backups / Archives | Client-side encryption before upload | Unencrypted cloud storage | Verify restore operations preserve encryption |
| Clinical Email | TLS 1.2+ / S/MIME | Plaintext exposure in transit | Deploy automated encryption gateways |
That kind of visibility turns policy from a paper exercise into something teams can enforce day to day.
A Practical Encryption Framework for Emergency Healthcare
After the standards and governance model, the next step is turning them into something teams can use day to day. HIPAA treats encryption as risk-based, but in emergency care, strong encryption should be the default starting point. In plain terms, most ePHI systems in emergency healthcare should be treated as if encryption is mandatory.
A simple way to put this framework into practice is to work across four layers.
- Know where ePHI lives and how it moves. Start with a full inventory before picking any control. That means databases, backups, mobile devices, APIs, and connected medical equipment. Each one brings its own risk.
- Set a clear encryption baseline. Use AES-256 for data at rest and TLS 1.3 or hardened TLS 1.2 for data in transit, with FIPS 140-3 validated modules across the stack.
- Build for clinical speed. Security can't slow down care. Use low-friction controls like FDE and TDE, and support them with break-glass procedures that are time-limited and audited.
- Keep watch all the time. Rotate keys every 90 days, retain audit logs for six years, and run annual risk analyses.
The stakes are hard to ignore. In 2024, HHS OCR logged 725 breaches involving 500 or more records, exposing about 276.8 million records - roughly 81% of the U.S. population [5]. That number makes the case on its own.
There’s also a direct compliance angle. Encrypted ePHI can qualify for HIPAA safe harbor if the keys stay protected. So if a laptop goes missing or a device is stolen, that event may not trigger mandatory breach notification under the HIPAA Breach Notification Rule [4][2].
The last gap is third-party oversight. Vendors, business associates, and connected devices need to meet the same encryption bar as internal systems. That work should be written into BAAs, checked through technical evidence, and watched over time. For vendor oversight, Censinet RiskOps™ helps centralize encryption evidence across vendors, applications, and medical devices.
FAQs
Is HIPAA encryption mandatory for emergency healthcare?
Yes. As of 2026, HIPAA-compliant encryption is required for all electronic protected health information (ePHI) in emergency healthcare.
That means encryption applies to both:
- Data at rest: use AES-256 for stored data
- Data in transit: use TLS 1.2 or higher for transmitted data
And here's the key point: there are no exceptions or risk-based bypasses, even during declared emergencies.
What systems should be encrypted first in an emergency care setting?
First, lock down every system that stores or sends electronic protected health information (ePHI).
Start with the devices and systems most likely to be exposed, especially mobile carts, laptops, tablets, and triage or registration workstations. Those endpoints should use full-disk encryption.
You should also encrypt key databases at rest, including EHRs, lab systems, imaging archives, and backups.
For data moving across your network, use TLS 1.2+ across the board, including for APIs and patient portals, so information stays protected in transit.
Does encrypted ePHI always avoid breach notification after a lost device?
Not always.
Encrypted ePHI may fall under the breach notification safe harbor in 45 CFR 164.402. But that only works if the encryption meets NIST-approved standards and the encryption keys stay secure.
Here’s the catch: if an unauthorized party can get both the encrypted data and the decryption keys, the safe harbor no longer applies. At that point, the incident may count as a reportable breach.
