If you can’t show who changed what, when, and from where, your audit trail may not help when it matters most.
I’d boil this down to a simple point: HIPAA audit trails are not just about logging access. They are about proving that ePHI was not changed, deleted, or mishandled without permission. That means logs must be complete, protected from editing, kept for at least 6 years, and actually reviewed. If they fail in any of those areas, patient care, audits, and breach reviews all get harder. This complexity makes measuring cybersecurity performance essential for maintaining safety.
Here’s the short version:
- HIPAA requires both logging and review under 45 C.F.R. § 164.312(b)
- Data integrity controls are also required under 45 C.F.R. § 164.312(c)
- A useful audit trail should show:
- who
- what
- which record
- when
- where
- success or failure
- Common weak points include:
- disconnected systems
- bad timestamps
- missing user mapping
- editable log storage
- short retention periods
- OCR penalties can range from OCR penalties can range from $100 to $50,000 per violation00 to $50,000 per violation, with annual caps up to $1.5 million per violation category
- The fix is plain:
- set one logging standard across systems
- use tamper-evident or write-once storage
- sync time with NTP
- review logs on a set schedule
- track gaps through closure
That’s the core idea: logs only matter if you can trust them, retrieve them, and use them to explain a record change fast.
What follows is a clear look at where audit trails break down, what HIPAA expects, and what I’d put in place to make the trail usable during audits, investigations, and care-related reviews.
What is an Audit Trail in Healthcare? (Explained - 2026)
sbb-itb-535baee
The Core Problem: Why Audit Trails Often Fail to Protect ePHI Integrity
Building a compliant audit trail sounds simple on paper. In practice, it often falls apart. Healthcare teams deal with disconnected systems, weak setup, and huge piles of log data. That mix makes it hard to prove ePHI integrity when someone asks for proof.
Most failures land in three areas: fragmented systems, poor configuration, and log volume.
Fragmented logging across EHRs, portals, medical devices, and vendors
Most healthcare organizations don’t work from one system. A typical setup may include EHRs, patient portals, PACS/RIS imaging systems, cloud apps, and vendor-managed services. Each one may log activity in a different way.
Some tools export JSON. Others use CEF. Older systems may not connect to modern centralized logging tools at all. And vendor-managed SaaS platforms often give covered entities only partial visibility into what the vendor tracks behind the scenes.
That creates a basic problem: no full chain of events.
Without that chain, teams can’t prove when a record changed or who changed it. If access and edit history is incomplete, no one can show whether ePHI was changed before entry or after it. And once those gaps show up, trust in the rest of the log data starts to slip. A timestamp might be off. A user identity might be unclear. A field-level change might be missing.
Misconfigured logs and weak review processes
Even when logging is turned on, the data may still be incomplete or shaky. In many audits, logs show that access happened, but not which fields were viewed or changed.
Five common failure points drive most of these gaps:
- missing human identity mapping
- non-UTC timestamps
- mutable log storage
- endpoint-only logging instead of resource-level logging
- retention shorter than six years
If a log can’t tie together the user, the record, and the timestamp, it can’t prove that the data stayed intact. That’s the heart of the issue.
There’s also a second problem that gets less attention: logs that no one reviews. Collecting data is not enough. Organizations must examine activity, not just record it [5]. If no one checks for odd access, missing entries, or broken time sync, the audit trail becomes a giant file cabinet that no one opens until it’s too late.
At that point, the issue isn’t just logging. It’s also archive and retrieval.
High-volume logging and six-year retention burdens
Volume is a plain old operations problem. Large academic medical centers can generate petabytes of log data every year [6]. Even a specialty practice with 1,000–5,000 active patients can build up tens of millions of audit rows over six years [5]. No team is going to review that by hand.
HIPAA requires audit documentation to be kept for at least six years from the date it was created. Some state laws go further. California requires seven years, and pediatric records in certain states must be kept for up to ten years [4][1][2].
That gets even messier during EHR migrations. When organizations move to a new platform, audit trails from retired systems often disappear in the handoff. That can become a retention violation by itself [5].
Long-term retention matters for a simple reason: if retrieval takes too long, the organization may struggle to prove integrity during an audit or breach review. When log sets get this big, storage is only part of the problem. Finding the right record fast enough is just as important.
The Solution: How to Build HIPAA-Compliant, Tamper-Resistant Audit Trails
HIPAA Audit Trail Compliance: Manual Review vs. Platform-Enabled Oversight
The fix comes down to three things: standardize the data, make the logs tamper-evident, and give someone clear responsibility for reviewing them.
Standardize what every system must log
Start by agreeing on what a complete log entry looks like across every system that touches ePHI [1][2].
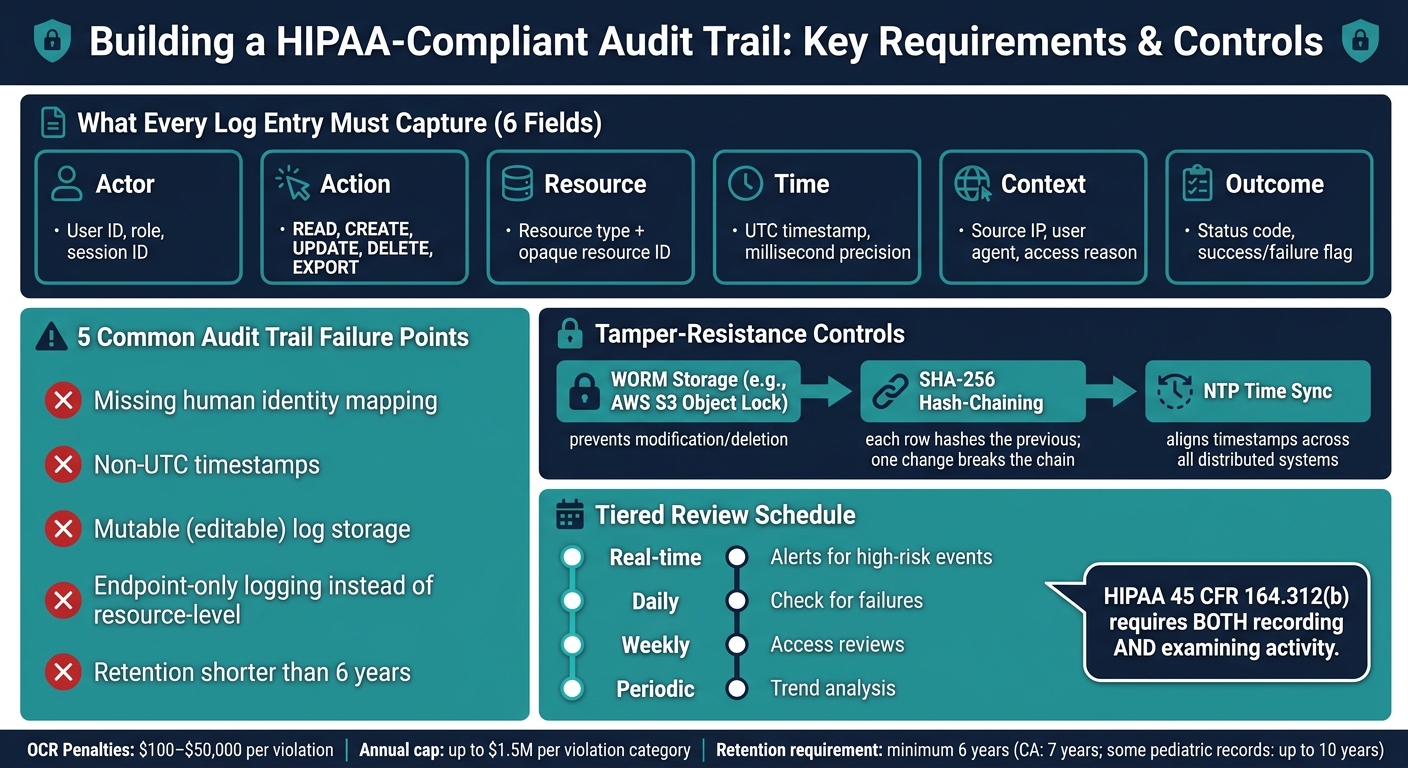
That means your EHRs, patient portals, medical devices, cloud systems, and vendor-managed environments should all record the same core fields:
| Field | What to Capture |
|---|---|
| Actor | User ID, role at time of access, session ID |
| Action | READ, CREATE, UPDATE, DELETE, EXPORT |
| Resource | Resource type, opaque resource ID (not patient name or SSN) |
| Time | UTC timestamp with millisecond precision |
| Context | Source IP, user agent, reason for access (e.g., treatment, break-glass) |
| Outcome | Status code, success or failure flag |
The log needs to identify the human user and any service account involved. It also needs to record the user's role at the time of access [1][2].
Using opaque resource IDs - internal database references like patient:1274 instead of names or Social Security numbers - helps keep the audit trail from turning into a PHI database of its own [1].
The 2026 HIPAA Security Rule also tightens expectations here. Organizations need evidence that logging controls are collecting the required fields [1][2].
Once the format is locked in, the next job is protecting the log store itself.
Protect logs from tampering and support investigations
A log only helps if you can show it wasn't changed after the fact.
Write-Once-Read-Many (WORM) storage - such as AWS S3 Object Lock - stops anyone from modifying or deleting a log entry after it has been written. Add cryptographic hash-chaining on top of that, where each log row includes a SHA-256 hash of the previous row, and you get a clear tamper-evident chain. Change one entry, and every hash after it breaks [5][1].
Nightly integrity checks help catch trouble early, before a SOC 2 audit or security event puts the logs under a microscope.
Time sync matters just as much. Every system should use an authoritative NTP source so timestamps line up well enough to rebuild event timelines across distributed environments.
Access to the logs also needs tight control. A one-way write path managed by compliance helps separate duties. In plain terms, IT admins shouldn't be able to edit records of their own activity. That makes the audit trail much stronger during an investigation.
The point is simple: preserve a defensible record of who changed what, when it happened, and whether the trail stayed intact.
Immutable logs don't do much good, though, if nobody looks at them.
Operationalize review, alerting, and staff accountability
HIPAA 45 CFR 164.312(b) requires both recording activity and examining it [5].
A tiered review model works well here:
- Real-time alerts for high-risk events
- Daily checks for failures
- Weekly access reviews
- Periodic trend analysis
Documented escalation paths matter too. Break-glass events should trigger immediate supervisor alerts and require a justification code [7][2]. That's the layer of accountability that turns a plain log file into usable evidence when someone needs to explain a record change.
Scaling Audit Trail Risk Management with Censinet
Even strong logging controls can fall apart when teams can’t spot gaps across EHRs, devices, cloud workflows, and vendor systems. That’s where centralized risk management helps.
Centralized visibility into audit trail gaps and related risks
Censinet RiskOps™ gives healthcare organizations one place to track audit trail-related findings across clinical applications, medical devices, PHI workflows, and vendor environments. Instead of running separate assessments that each show only part of the picture, the platform pulls findings into centralized dashboards with real-time visibility [8].
Audit data isn’t captured the same way in every system. One platform may log one set of events, while another records something else entirely. Without a standard way to compare those records, enterprise-wide review gets messy fast.
Collaborative workflows for remediation and vendor accountability
When a gap shows up - like missing six-year retention or missing modification records - Censinet RiskOps sends it to the right internal owner or vendor and tracks it through closure [3][6]. That shifts audit trail review from a manual back-and-forth into a managed workflow.
Manual review vs. platform-enabled oversight with Censinet
Platform-enabled oversight cuts down on manual log chasing, shortens audit response time, and puts accountability in one place.
Conclusion: How Continuous Audit Trail Improvement Strengthens Compliance and Trust
Audit trails are not a one-time control. They protect data integrity only when logging, storage, review, and accountability all work together. When the trail is complete and reviewable, it becomes proof that ePHI was not altered without authorization. The clearest sign that this is working is measurable performance.
The 2026 HIPAA Security Rule makes audit-control review an ongoing requirement. That matters because audit controls are how organizations show that the record stayed intact. Auditors want testable evidence that logging is active, complete, and reviewable - not just written in a policy.[1][2] That’s why the right metrics matter.
Metrics that show whether audit trails are working
Use metrics to check that the controls are doing their job. These five metrics help verify audit trail performance.
| Metric | Audit Trail Data Source | Leadership Decision Support |
|---|---|---|
| Mean Time to Detect (MTTD) | SIEM / Alerting Logs | Shows response speed |
| % of Systems Meeting Logging Standards | Centralized Log Management Dashboard | Shows coverage gaps |
| Unresolved Audit-Related Findings | Compliance Dashboard / Risk Register | Shows remediation backlog |
| Audit Retrieval Success Rate | Cold Storage / Archive Restoration Logs | Verifies restorability |
| Unauthorized Access Rate | Triage / Investigation Outcomes | Signals privacy risk |
Tracking these metrics over time shifts audit trail management from a reactive exercise to a governance function that leadership can actually use. If the share of systems meeting logging standards goes up, remediation is moving in the right direction. If mean time to detect goes down, monitoring is getting sharper. Put together, these numbers give leaders a clear view of where the program stands - and where gaps still need work.
FAQs
How do audit trails support HIPAA data integrity?
Audit trails help support HIPAA data integrity by keeping a chronological, tamper-evident record of ePHI activity. They show who accessed data, what changed, when it happened, where the action came from, and why it took place.
For compliance, logs should live in immutable formats, such as append-only or WORM storage. They should also be protected with cryptographic hashes so no one can change or delete them without detection.
What makes an audit trail tamper-evident?
An audit trail is tamper-evident when it blocks unauthorized changes and makes any later edit easy to spot.
Teams usually do this with append-only or WORM storage, plus cryptographic methods like hash chaining or digital signatures. Here’s the basic idea: if someone changes a record after the fact, the chain breaks. That break signals that something was altered.
Restricted access also matters. So does continuous monitoring. Those controls help keep the trail trustworthy.
How often should HIPAA audit logs be reviewed?
HIPAA requires regular audit log reviews to spot suspicious activity and support compliance with the Activity Review standard. There isn’t one fixed review schedule for every organization, though the 2026 Security Rule update makes annual reviews mandatory.
In practice, review timing should come from a formal risk analysis, your team’s operational maturity, and the current threat landscape. A common approach looks like this: continuous alerting for high-risk systems, weekly reviews for moderate-risk systems, and monthly reviews for lower-risk systems.
